
apoE4 and Genetic Mediated Risk of Alzheimer’s
May 25, 2018
-
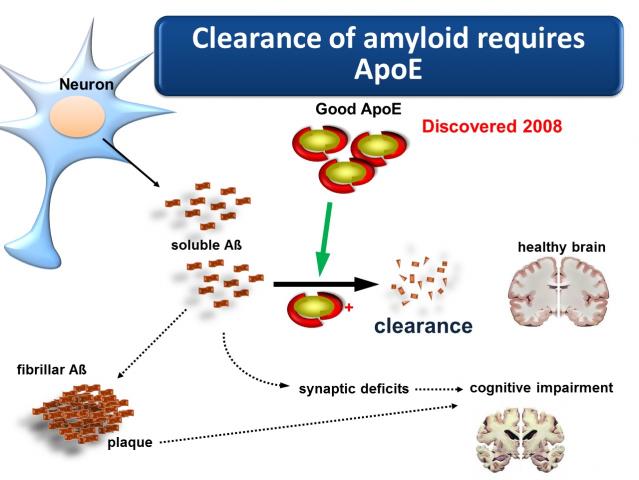
apoE is an apoprotein and one of its major jobs is helping to remove a major abnormal protein that is continually being made in the brain called beta amyloid, which when it is build up in the brain it is a primary mechanism involved in Alzheimer’s disease and other forms of dementia
-
By age 65 approximately 1 in 6 persons will develop the disease with the risk increasing progressively with age. The apoE 3 genotype is most common and is used to predict relative risk of the disease
-
The risk with apoE 2/2 is reduced 40% compared to apoE 3. Having one apoE 4 gene increases risk between 2 ½ and 3 ½ times. The apoE 4/4 genotype increases the risk 15 to 20 times
-
The onset of symptoms such as memory loss do not occur until significant loss of brain volume has occurred.
-
Given the rapid increase in the rates of Alzheimer’s disease it is wise to have genetic risk testing early
apoE is an apoprotein which means that it is a protein structure that helps to transport fats such as cholesterol. However, it has several other functions which are important to all tissues including the brain. One of its jobs is helping to remove a major abnormal protein that is continually being made in the brain called beta amyloid. Beta amyloid build up in the brain is a primary mechanism involved in Alzheimer’s disease and other forms of dementia. The excessive build-up of beta amyloid in the brain is a major cause of the degeneration neurons and their connection to other neurons which leads to loss of brain volume and function. Certain genetic variations in apoE cause it to be heavily impaired in its ability to remove beta amyloid.
apoE is made by a gene located on chromosome 19 and has three different forms: apoE 2, apoE 3, and apoE 4. The apoE 4 variety greatly increases the risk of developing Alzheimer’s disease.
As each of us has two copies of the gene, each person may have one of several combinations of the 3 types of apoE. Having two copies of the same apoE such as apoE3/3 is called homozygous, while having two different copies such as apoE 3/4 is heterozygous. The functional apoE can be made from either gene so at any time the available apoE can be some good and some bad in someone heterozygous with one higher risk gene and one lower risk gene. Being homozygous with two lower risk copies lowers the risk more than having only one lower risk copy. Similarly, risk is greatly increased with two copies of the high risk gene such as apoE 4.
The apoE 2 genotype is the most protective against Alzheimer’s but only 7% of the population is apoE 2/2. The highest risk group for Alzheimer’s disease is the apoE 4/4 genotype. This genotype is present in about 15% of the population with another 15-20% having one copy of apoE 4.

By age 65 approximately 1 in 6 persons will develop the disease with the risk increasing progressively with age. The apoE 3 genotype is most common and is used to predict relative risk of the disease.
The risk with apoE 2/2 is reduced 40% compared to apoE 3. Having one apoE 4 gene increases risk between 2 ½ and 3 ½ times. The apoE 4/4 genotype increases the risk 15 to 20 times.
Most genetic mediated disease associations are “polygenic” meaning that there are multiple gene abnormalities in addition to apoE which occur in the same person contributing to the overall risk. This is why some studies looking only at the increased risk associated with apoE4/4 find the risk is increased 10x and others find it is increased by 20x. These other factors are being discovered and will contribute to the analysis in the progressive future, but the apoE type remains the single greatest genetic risk factor.
A key point to understand in the assessment of real life risk is that the genetic factors do not independently trigger the disease. The process also involves the presence of environmental stressors which are largely lifestyle related. Not everyone with the apoE 4 genotype will develop the disease, and a significant number of persons with the lower risk genotypes will still develop it. The genetic factors appear to make certain persons less tolerant to the different stressors that imbalanced lifestyle generates. In essence, the higher risk genetic persons require much tighter lifestyle control to minimize the risk.
Lifestyle is completely modifiable and should form the basis of risk modification. Family history is also an important variable being driven both by genetic and by lifestyle related factors. It tends to have perhaps more positive predictive value than negative predictive value. This simply means that if someone’s family history is positive, risk is greatly increased; but if it is negative, they are not necessarily protected. We have seen progressive increases over the past 50 years in the lifestyle related factors and the diseases they drive such as overweight and diabetes. The presence of several strong factors in the same person may trigger degenerative brain disease risk in the absence of genetic risk.
One additional important factor in risk evaluation is timing. The interaction between the lifestyle driven factors such as high inflammatory markers or high insulin levels cause the progressive injury to the brain over several decades. The onset of symptoms such as memory loss do not occur until significant loss of brain volume has occurred. The ideal risk reduction program should involve evaluation of genetic and potential triggering lifestyle related factors in mid-life when the cellular level damage is beginning.
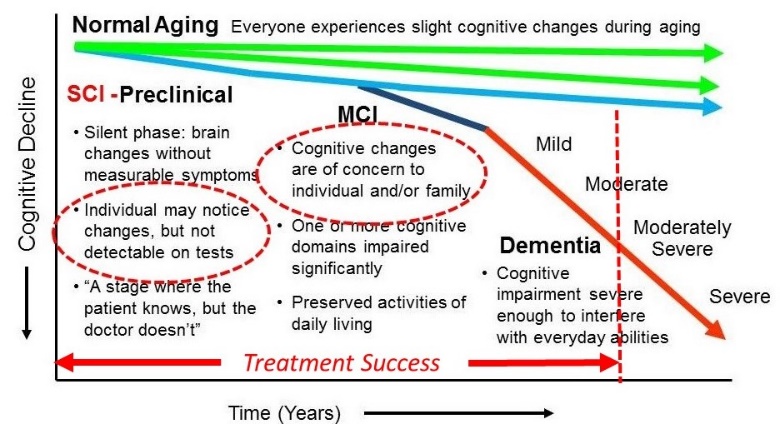
Very forward thinking treatment programs such as the Bredesen Protocol have demonstrated high levels of success in the earlier stages of the process. The first symptomatic phase is SCI, or subjective cognitive impairment. In this phase the individual notices some memory deficit, but it is not to the degree that is readily apparent to others. The next stage is MCI or minor cognitive impairment where the symptoms can now be noticed by others close to the individual, but they do not interfere with normal basic functioning. Once the diagnosis of early Alzheimer’s is made, the individual has begun to lose some ability to normally function such as working, being able to remember where they are and get where they are going and other similar problems.
The point at which progressive lifestyle management programs become less successful appears to be between mild and moderate Alzheimer’s disease when the impairment has grown enough that evaluation is sought. Given the rapid increase in the rates of Alzheimer’s disease it is wise to have genetic risk testing early. If positive genetic risk is combined with a positive family history, extensive testing of lifestyle related risk factors should be undertaken and targeted lifestyle interventions should be implemented. Genetics are “unfair” as we have no choice in the matter. Fortunately, lifestyle is the opposite, we all have a choice.
